
We present the case of a 91-year-old man with a past medical history of moderate-to-severe aortic stenosis referred due to breathlessness. The routine invasive coronary angiography performed before transcatheter aortic valve replacement confirmed the presence of a severely calcified left anterior descending coronary artery proximal segment (figure 1A; video 1 of the supplementary data). The functional assessment performed showed a fractional flow reserve of 0.79. The optical coherence tomography (OCT) interrogation revealed an arc of calcium > 180°, thickness of 0.6 mm, and length > 5 mm with a calcified nodule with a minimum lumen area of 3.49 mm2 (figure 1C; video 2 of the supplementary data). Orbital atherectomy with the Diamondback 360 Coronary OAS (Cardiovascular Systems, Inc., United States) was selected to prepare the lesion. After 5 runs at low speed (80 000 rpm), a new OCT was performed that confirmed the fracture of the calcified nodule achieving a minimum lumen area of 7.5 mm2 (figure 1D; video 3 of the supplementary data). Consecutively, a 2.5 mm x 15 mm SC balloon (OrbusNeich, China) plus a 3.0 mm x 10 mm NC balloon (Medtronic, United States) were advanced through the lesion and inflated twice. Finally, a Megatron 3.5 mm x 20 mm drug-eluting stent (Boston Scientific, United States) was implanted at 20 atm. Both the post-stenting final coronary angiogram (figure 1B; video 4 of the supplementary data) and the OCT pullbacks confirmed the homogeneous expansion and correct apposition of the stent (figure 1E; video 5 of the supplementary data). All the pertinent informed consents were obtained.
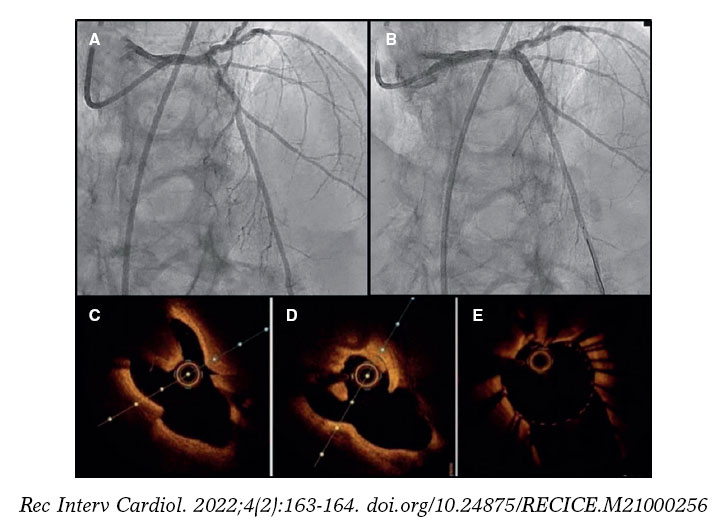
Figure 1.
We presented one of the first cases of orbital atherectomy as an effective tool to treat calcified nodules, and the first case of revascularization supported not only by angiography, but also by intracoronary imaging.
FUNDING
None reported.
AUTHORS’ CONTRIBUTIONS
All authors participated in the process of drafting this manuscript. Also, all the authors approved its final version.
CONFLICTS OF INTEREST
None of the authors declared any conflicts of interest in association with this manuscript.
SUPPLEMENTARY DATA
Vídeo 1. Abellas-Sequeiros M. DOI: 10.24875/RECICE.M21000256
Vídeo 2. Abellas-Sequeiros M. DOI: 10.24875/RECICE.M21000256
Vídeo 3. Abellas-Sequeiros M. DOI: 10.24875/RECICE.M21000256
Vídeo 4. Abellas-Sequeiros M. DOI: 10.24875/RECICE.M21000256
Vídeo 5. Abellas-Sequeiros M. DOI: 10.24875/RECICE.M21000256
E-mail address: maine.iaca@gmail.com (M. Abellas-Sequeiros).










