
A 52-year-old woman was admitted due to ischemic stroke treated with mechanical thrombectomy. She reported having a fever in the previous month, and a continuous systolic-diastolic murmur was identified during auscultation. An echocardiogram revealed the presence of a 7 mm x 5 mm persistent patent ductus arteriosus with hemodynamic repercussions (overload of left heart chambers) (figure 1A,B, arrow; videos 1 and 2 of the supplementary data). Additionally, a wart was found on the aortic valve with mild regurgitation. Streptococcus sanguinis was found in blood culture isolates. The thoracic coronary computed tomography angiography not only characterized the ductus, but also showed a vegetation on the pulmonary trunk, along with septic pulmonary emboli (figure 2A,D, arrow). A 4-week course of antibiotics was initiated. Due to worsening echocardiographic findings (vegetation growth, and progression of regurgitation) (figure 1C,D; videos 3 and 4 of the supplementary data), surgical intervention was decided to replace the aortic valve with a mechanical valve and close the ductus with a patch.
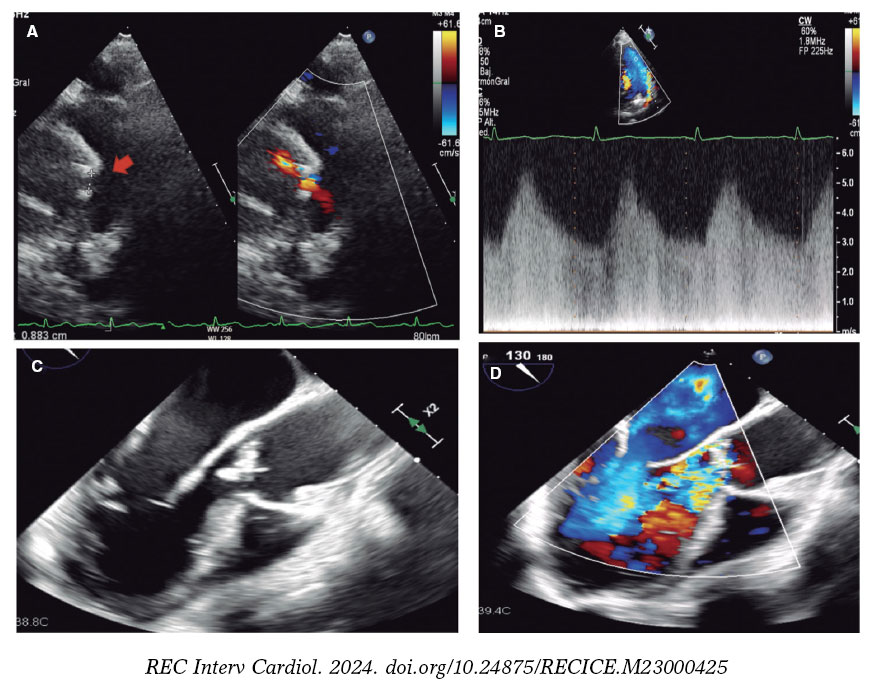
Figure 1.
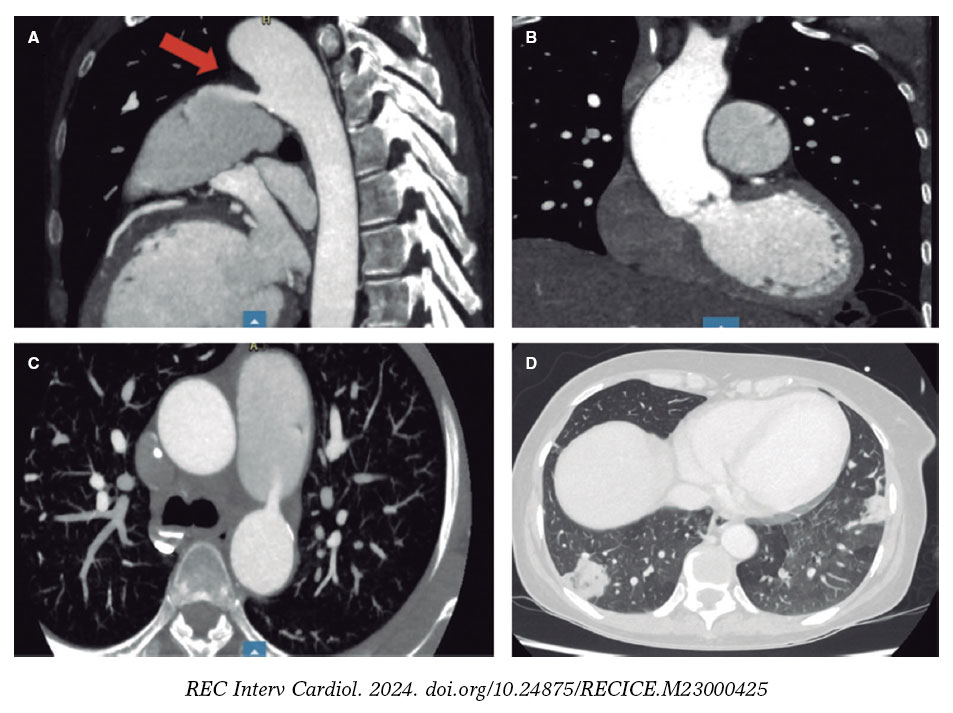
Figure 2.
In adults, the ductus can become calcified, thus hampering simple ligation. In this case, a small residual shunt remained, which was closed percutaneously 6 months later, following confirmation of the absence of inflammatory activity on positron emission tomography/computed tomography. After descending aorta angiography, crossing the ductus proved challenging because of its tortuosity and the presence of the patch. Microcatheter support and a 2.5-mm angioplasty balloon were used to finally implant an Amplatzer Duct Occluder II device (Abbott, United States) (figure 3A,B,J, arrow; videos 5 and 6 of the supplementary data).
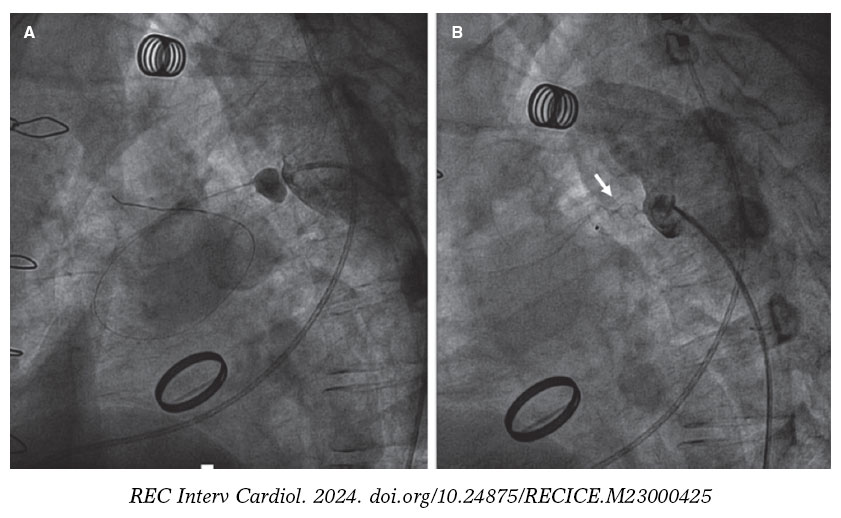
Figure 3.
The ductus is a rare cause of endocarditis because the turbulent flow jet causes endothelial damage that promotes bacterial invasion. “Preventive” closure of silent ducts is not included in clinical practice guidelines but is recommended by some groups recommend because it is a low-risk procedure.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
Informed consent was obtained from the patient to publish her case. Since this is an isolated case report, most SAGER guidelines do not apply. The patient’s gender (woman) has been specified. However, since this is a case report and not a research study, additional considerations were not deemed necessary.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used.
AUTHORS’ CONTRIBUTIONS
A.T. Ariza, and P. Merás Colunga drafted the initial version of the manuscript, and selected and edited the images that would later be used. C. Merino, J. Ruiz Cantador, and R. Moreno were involved in the manuscript critical review, and approved its final version. I. Pinilla acquired the computed tomography images and approved the final version of the manuscript.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. No other conflicts of interests are declared.
MATERIAL ADICIONAL
Vídeo 1. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425
Vídeo 2. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425
Vídeo 3. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425
Vídeo 4. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425
Vídeo 5. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425
Vídeo 6. Tatiana Ariza A. DOI: 10.24875/RECICE.M23000425










