
We present the case of a 12-year-old boy treated for a secundum atrial septal defect (sASD) at the age of 2 years who was referred due to dyspnea, cyanosis with digital clubbing, and oxygen desaturation of 75%.
Transthoracic echocardiogram showed an acceleration of flow of the inferior vena cava (IVC) inside the right atrium (RA) due to an iatrogenic suture between the Eustachian valve and the upper part of the ASD, with residual right-to-left shunt.
Subsequently, a transesophageal echocardiogram and cardiac catheterization (figure 1, arrows) with cavogram revealed the severe obstruction of the IVC drainage into the RA through a 6 mm orifice, with a 12 mm IVC diameter, and a residual 5 mm ASD, leading to a right-to-left shunt (videos 1-3 of the supplementary data).
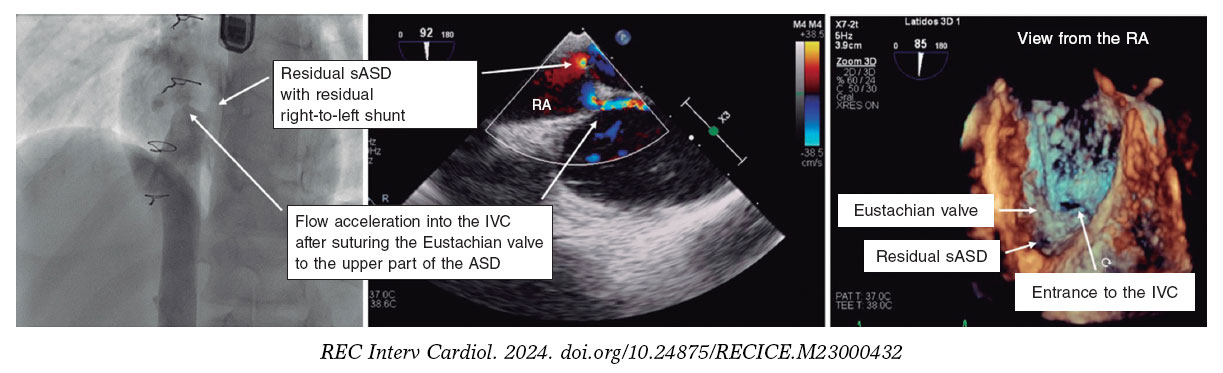
Figure 1.
The cava axis was catheterized, and the stenosis area was sequentially dilated with balloons of up to 22 mm. Color Doppler echocardiography confirmed the absence of flow acceleration, and a hemodynamic gradient of 1 mmHg between the IVC and the RA. A 4 mm occlusion device was implanted to close the ASD without residual shunting after its release (figure 2, arrows), resulting in the restoration of normal oxygen saturation.
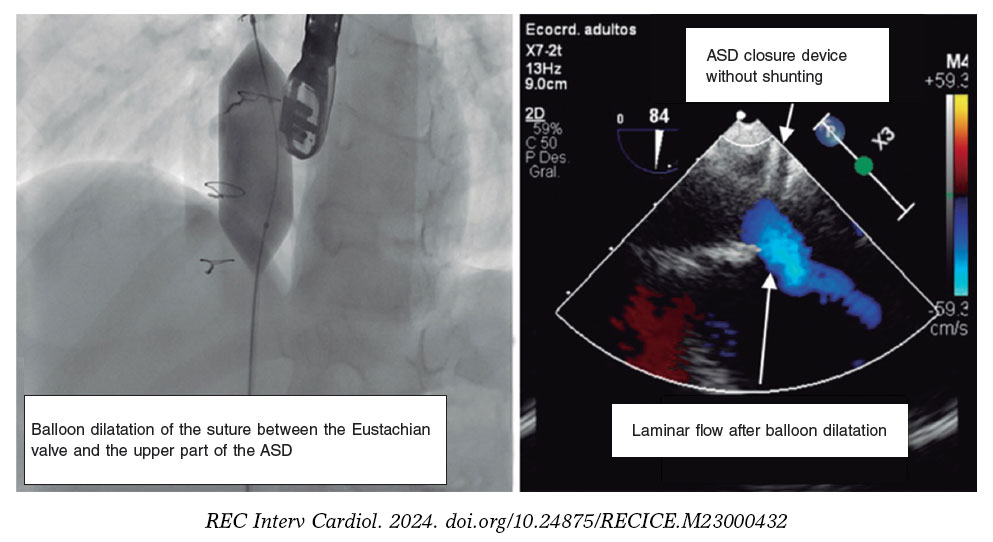
Figure 2.
The partial deviation of the IVC into the RA can occur iatrogenically after surgical closure of an sASD by suturing the Eustachian valve to the upper part of the ASD. The standard of care for this complication is usually surgical reintervention. This is the first case ever reported of an obstruction treated with balloon dilatation.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This article abides by the international recommendations on clinical research. Considering the content of the article, it was not deemed necessary to account for potential sex and gender biases. The patient’s prior written informed consent form was obtained for publication.
DECLARATION ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools have been used.
AUTHORS’ CONTRIBUTIONS
All authors were physicians of the patient and contributed to the drafting of this article.
CONFLICTS OF INTEREST
None declared.
SUPPLEMENTARY DATA
Vídeo 1. Arreo del Val V. DOI: 10.24875/RECICE.M23000432
Vídeo 2. Arreo del Val V. DOI: 10.24875/RECICE.M23000432
Vídeo 3. Arreo del Val V. DOI: 10.24875/RECICE.M23000432
* Corresponding author.
E-mail address: vivi.arreo@gmail.com (V. Arreo del Val).









