
CASE RESOLUTION
The outcome was successful with a final 19-mmHg intraventricular gradient and after the extrasystole of 25 mmHg (figure 1). No more new events of ventricular tachycardia (VT) were reported, disease progression was good, and the patient remained asymptomatic at 3 months.
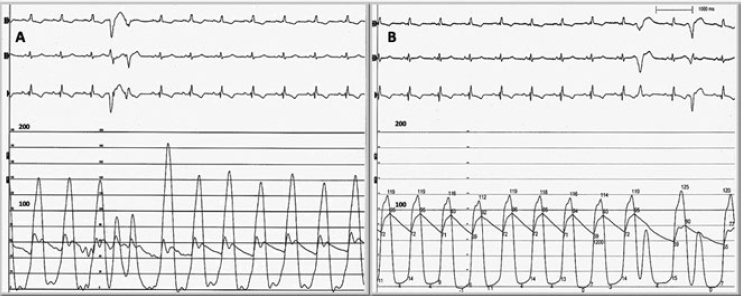
Figure 1. A: gradient between left ventricle and initial aorta. B: gradient between left ventricle and final aorta.
Sustained monomorphic VT in hypertrophic cardiomyopathy is a rare entity. These patients are considered eligible to receive an automated implantable-cardioverter defibrillator and antiarrhythmic drugs. Also, in cases of VT of focal origin, the mapping of cardiac electrophysiology and ablation is indicated. In 1989, Brugada et al.1 first published that in the management of patients in whom other options have failed, alcohol ablation of the coronary branches that irrigate the origin or route of VT is a valid therapeutic option to treat persistent tachycardia.
Our case is unique because it describes the role of septal ablation for arrhythmic and hemodynamic control purposes in a septal region where the maximum gradient and origin of VT were located. Even though septal ablation can be less effective in large scars and hypertrophies ≥ 30 mm, it can also be a successful procedure and replace myectomy in high risk patients or centers with low surgical experience with similar long-term mortality rates for both strategies. Bubble contrast echocardiography is effective to enhance the region perfused by the target branch with the corresponding lower use of alcohol and fluoroscopy. The ablation of VT in hypertrophic cardiomyopathy is successful in up to 80% of the cases2; however, sometimes its utility is limited because the ventricular wall is too thick and there is an unreachable deep intramural reentry circuit. Magnetic resonance imaging is useful in the electrophysiological search of the circuit and to help identify the size, location, and thickness of the scar. When radiofrequency ablation fails in the management of VT, as it was the case here, alcohol ablation can prevent recurrences and improve control.3 In conclusion, it is a good alternative to treat refractory VT during the management of hypertrophic cardiomyopathy.
REFERENCES
1. Brugada P, de Swart H, Smeets JL, et al. Transcoronary chemical ablation of ventricular tachycardia. Circulation. 1989;79:475-482.
2. Dukkipati SR, Koruth JS, Choudry S, et al. Catheter Ablation of Ventricular Tachycardia in Structural Heart Disease. J Am Coll Cardiol. 2017;70:2924-2941.
3. Kumar S, Barbhaiya CR, Sobieszczyk P, et al. Role of Alternative Interventional Procedures When Endo and Epicardial Catheter Ablation Attempts for Ventricular Arrhythmias Fail. Circ Arrhythm Electrophysiol. 2015;8:606-615.
Corresponding author: Juan Badiano 1, Col. Belisario Domínguez, Sección XVI, 14080 Tlalpan, Mexico City, Mexico.
E-mail address: custodiomed@hotmail.com (P. Custodio-Sánchez)









