
Eighty-five-year-old woman with unstable angina with serious and heavily calcified lesions in proximal right coronary arteries (figure 1A, asterisk) and proximal and mid left anterior descending coronary artery (figure 1B, asterisk).
Rotational atherectomy was performed in the right coronary artery using the RotaPro system (Boston Scientific, United States) (figure 1C) and a drug-eluting stent was implanted with good results (figure 1D) as confirmed by the intracoronary ultrasound (figure 1E). Informed consent was obtained from the patient.
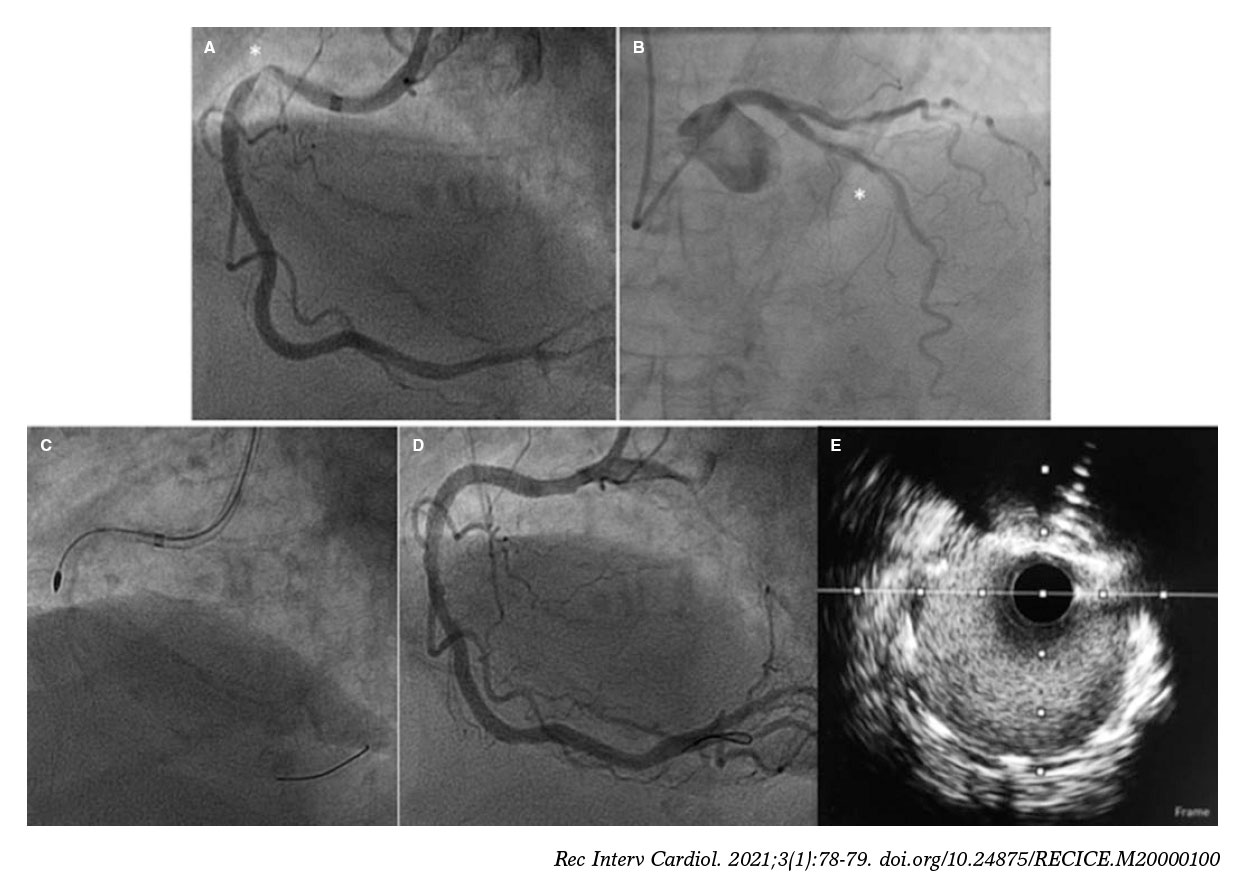
Figure 1.
After the catheterization of the left main coronary artery (LMCA) the left anterior descending coronary artery was crossed. A 1.5 mm olive-shaped burr was advanced in the DynaGlide mode towards the LMCA, which is when the guide catheter was extubated and an Ellis type III perforation occurred in the LMCA (figure 2A, asterisk; video 1 of the supplementary data); it is possible that an unnoticed deformation of the guidewire moved the burr towards the vessel wall. The patient showed cardiac tamponade that was treated with pericardiocentesis. A 4 × 15 mm PK-Papyrus covered coronary stent (Biotronik, Germany) was implanted in the LMCA without jailing the bifurcation (figure 2B). However, a discrete leak of contrast still occurred (figure 2C, asterisk). After postdilatation with a 4.5 mm balloon, the perforation was sealed (figure 2D; video 2 of the supplementary data). The disease progression of the patient was favorable.
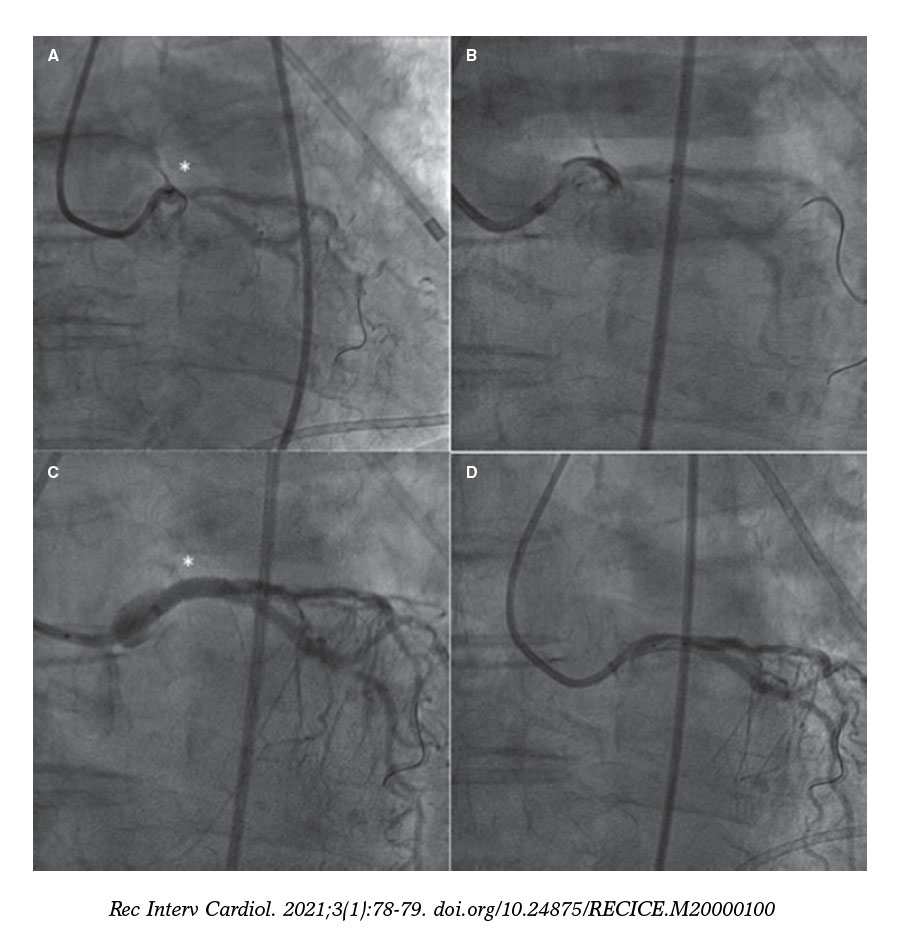
Figure 2.
Coronary perforations at LMCA level are rare, but they can be lethal. Prolonged balloon inflations in this location are not well tolerated, which is why proceeding to implant the covered stent fast may be the best alternative. To our knowledge, this is the first perforation of the LMCA ever reported with rotational atherectomy resolved with a Papyrus stent.
FUNDING
No funding.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed.
SUPPLEMENTARY DATA
Video 1. Jurado-Román A. DOI: 10.24875/RECICE.M20000100
Video 2. Jurado-Román A. DOI: 10.24875/RECICE.M20000100
Corresponding author: Servicio de Cardiología, Hospital Universitario La Paz, Paseo de la Castellana 261, 28046 Madrid, Spain.
E-mail address: alfonsojuradoroman@gmail.com (A. Jurado-Román).










