
An 80-year-old male with permanent atrial fibrillation (informed consent obtained) underwent a percutaneous procedure to close the left atrial appendage (LAA). He had required repeated admissions for severe anemia and chronic gastrointestinal bleedings while on different antithrombotic regimens (aspirin alone, clopidogrel alone, apixaban). He had a CHADS-VASC2 score of 6 and a HAS-BLED score of 4. A transesophageal echocardiography (TEE) performed revealed the presence of Windsock morphology and no thrombus in the LAA. The diameters of the landing zone were between 23 mm and 25 mm (figure 1).
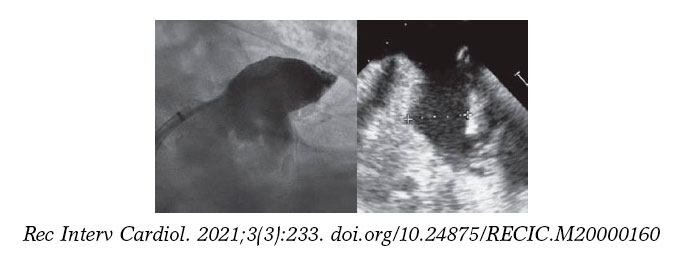
Figure 1.
A 28-mm Amulet device was chosen to perform the procedure. A 14-Fr introducer sheath was advanced into the left atrium and, after a selective angiography, the device was deployed inside the LAA in a regular fashion. The first deployment did not achieve a good position (partially outside the appendage) and the device had to be recaptured. A second attempt was made with significant counterclockwise rotation of the sheath that achieved a peculiar “twisted” deployment of the body of the device (figure 2) whose distal part was actually deployed inside the appendage. It was carefully recaptured and after discarding pericardial effusion, it was re-implanted in a good position this time with no further need to change the device (figure 3). A transthoracic echocardiography performed the next day revealed no pericardial effusion. The TEE performed 1 month later revealed no leaks or thrombi on the device either.
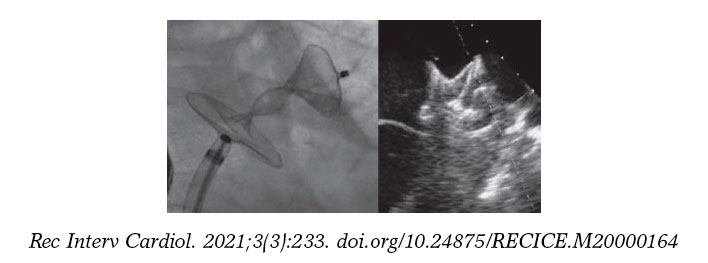
Figure 2.
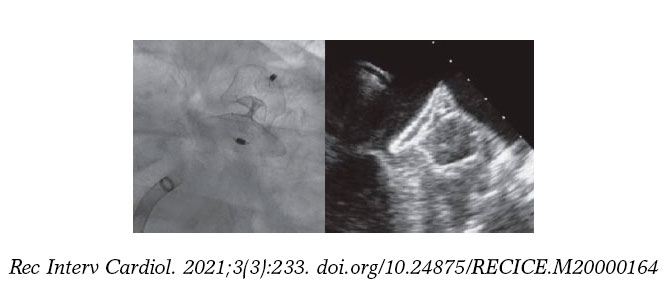
Figure 3.
The immediate complications described with LAA occluding devices are embolization, incomplete closure with residual leaks or the development of pericardial effusion and cardiac tamponade. Twisted malappositions are actually rare and could be predictors of short-term complications.
FUNDING
No funding source related to he manuscript.
AUTHORS' CONTRIBUTION
F. Hernández and E. Lázaro, procedure performance; all authors contributed in the drafting and revision of the manuscript.
CONFLICTS OF INTEREST
F. Hernández Hernández is a proctor for Abbott on issues concerning left atrial appendage occlusions.
Corresponding author: Departamento de Cardiología y Cirugía Cardiaca, Clínica Universidad de Navarra, Marquesado de Santa Marta 1, 28027 Madrid, Spain.
E-mail address: felipeivus@hotmail.com (F. Hernández Hernández).